I've been reading through an extremely eye-opening and concerning open letter sent to the Irish government from Ivor Cummins. I've copied it below. It's quite lengthy but definitely worth a read. I've had to split this into two messages as I can only attach ten documents.
'I am writing to you as I feel a patriotic duty to bring some focus back to the science and data around this Covid19 issue. The current approach that our government and advisory panels are driving, is increasingly inexplicable when considering the science and the data. It is becoming obvious that we need to foster more open discussion on the big picture here. Is there a good technical reason to continue with the current level of, quite frankly, destructive interventions?
Firstly, I would like to bring to your attention some basics in this matter (section A), and then back up the discussion with more detailed and referenced science (section B). The essence of this document is now agreed with by a very large (and rapidly growing) community around the world. Countless medical and technical professionals are at this stage, aghast at what is happening.
SECTION A – The Basics:
As the Epidemic morphed into a Pandemic as determined by the WHO, data from China, Italy, SE Asia, and other European countries gave us a clearer picture of how this particular virus was behaving. This data informed us regarding important aspects of Sars-CoV-2 including transmission, immunity, people most likely to succumb to the virus, ICU admission rates, death rates, seasonality, predisposing factors and much more.
The Global response to the pandemic, apart from some notable exceptions, was to as quickly as possible lock down our communities and our economies and flatten the curve, thus buying time to allow us deal with the sick and to continue the race for vaccines and therapies. This was an understandable and intuitive reaction and to some extent has been a success.
We’ve had ~27,000 cases, and sadly 1774 of our citizens have lost their lives, and my condolences to all their families and friends. That said, it is important to note that approximately 95% of the deceased were never admitted to ICU to attempt to save them. This is almost certainly because they were so aged or suffering from other serious conditions, that it would have been unethical to attempt to save them with intensive interventions. This, along with the fact that median age for the deceased was 83, must be kept clearly in mind when considering impacts.
At this point it is important to state a few indisputable facts that have emerged before and during this pandemic:
SARS-CoV-2 is a Coronavirus that shares many structural and behavioural properties with many other coronaviruses that affect human beings. This Coronavirus was referred to as novel. This is somewhat of a misnomer.
Face Masks at the height of the Pandemic were considered unimportant, we were regularly informed of this from experts through our media.
Covid 19 (the condition produced by Coronavirus) is a condition that predominantly affects the elderly and immunocompromised (as mentioned above, median age of death is 83yrs), it does not affect certain other groups like children and pregnant women in a way that Influenza, another seasonal killer, does.
A significant number of people succumb to Influenza virus each year, this can vary in its severity and impact; for example, the 2018 flu season was particularly severe in the UK, causing approximately 20,000 excess deaths in the month of January alone. The 2019 flu season was comparatively lighter, thus paving the way for a pathogen such as SARS-CoV-2 to heavily impact the susceptible in our population – a large group who would have ordinarily experienced higher mortality during the preceding Flu season.
The death rate has been similar throughout the World (approx. 500 (+/-) deaths per million). This, and I cannot emphasise this enough, is overwhelmingly independent of lockdown measures.
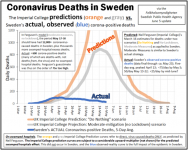
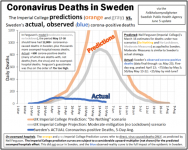
The reaction of most Governments has been largely based on the predictive models of Imperial College London. Experts in Ireland primarily used this model and the predictions made were mindboggling – one prominent Irish expert claimed that 42,000 deaths would have occurred, “one in every household in Ireland”, suggesting that the lockdown measures we implemented had saved 40,000 lives - and that the sacrifices of the Irish people were hence vindicated. The reality we now know was destined to be less than 1,800. We experienced a similar impact as Sweden did (they with no lockdown, no masks). Overwhelmingly it was limited to the aged / co-morbid, with care homes contributing to the majority of the deaths.
The following facts are also indisputable:
Sweden, who were vilified for their approach, has had a very similar death rate to other countries. Sweden enacted a light touch response to SARS-CoV-2 (smart social distancing, smaller crowds, emphasis on hand hygiene), while largely leaving their economy, including schools, open. According to the now heavily questioned Imperial College London model, Sweden should have had 11-17 times the number of deaths that it actually had. This has been backed up by studies and peer reviewed publications such as The Lancet. Hard lockdown has little impact on the death rates when compared to social distancing, hand washing, masks if symptomatic etc. This is a hugely important point. Sweden’s science-based policy has allowed them to emerge from the pandemic with many sectors of its economy and public health intact. It is close to achieving Herd Immunity, and all of this was possible without any lockdown.
Like most countries in Europe Sweden has little or no deaths or ICU admissions from Covid 19 in recent weeks, without requiring any of the measures imposed by the vast majority of European countries
Sweden is not on its own in following this course. There are some contrasting examples of hard lockdown v light touch response in the US and in South America. Peru imposed a hard lockdown while its neighbour Brazil was attacked in the media for their softer approach. Again, we see similar death rates from both. i.e. the military-enforced lockdown in Peru not showing any significant benefit over Brazil’s lack of any significant lockdown.
Sweden “modelling” versus actual reality is illustrated below:

Ref:
https://swprs.org/covid19-lethality-how-not-to-do-it/
SECTION B – The Details:
B1: EPIDEMIOLOGICAL REALITIES
2013 Nobel Laureate, Stanford Professor Michael Levitt
At this point it is important to invoke some fundamental mathematics and science.
Professor Michael Levitt, Nobel prize winner for Chemistry in 2013 and many other experts in epidemiology, have been deciphering the data provided by the viral spread. Professor Levitt has been interviewed a number of times over the last few months (notably on Irish television). He concluded that the curves produced by death rates were not exponential as per the Imperial College London models, and rather followed what is referred to a Gompertz phenomenon i.e. steep sharp rise followed by a flattening, followed by a long slow tail. This occurs as the virus “burns out” (the susceptible population pass, and ultimately a herd immunity develops). This has been the way countries have played out time after time. Notably, this behaviour mirrors influenza epidemic behaviour almost perfectly – this reality should have been the key focus since March. Please see example curves below. Remember, this is the actual
data – not modelling.
 Ref: “Predicting the Trajectory of Any COVID19 Epidemic From the Best Straight Line” - DOI: https://doi.org/10.1101/2020.06.26.20140814
Ref: “Predicting the Trajectory of Any COVID19 Epidemic From the Best Straight Line” - DOI: https://doi.org/10.1101/2020.06.26.20140814
There are endless references showing the seasonal Gompertz distribution of influenza epidemics – just one sample below – note the almost exact match with SARS-CoV-2 behaviour. This has been known for a century or more:
 Ref: “Time variations in the transmissibility of pandemic influenza in Prussia, Germany, from 1918–19” - Theoretical Biology and Medical Modelling volume 4, Article number: 20 (2007)
Ref: “Time variations in the transmissibility of pandemic influenza in Prussia, Germany, from 1918–19” - Theoretical Biology and Medical Modelling volume 4, Article number: 20 (2007)
Note also that one of the world’s top professors in epidemiology / evidence-based medicine (Stanford Prof John Ioannidis) called this out back in March 2020 – he was horrified at what the world was embarking upon, based on dreadfully poor evidence:

Ref:
https://onlinelibrary.wiley.com/doi/full/10.1111/eci.13222
MOST IMPORTANTLY, the impact of Covid 19 in Europe is not nearly what people perceive. As pointed out by Professor Levitt repeatedly, the excess mortality from Covid 19 is not very much greater than the excess mortality observed during the 2018 influenza season. The European mortality data can be pulled by anyone who cares to do so, and it tells a clear story of reality:

Ref:
https://www.euromomo.eu/graphs-and-maps
Note 1: The SARS-CoV-2 “season” was very short and sharp in its impacts, which is not surprising considering the very soft influenza seasons directly preceding SARS-CoV-2 in Europe.
Note 2: The impact seen could be challenged by claiming that “lockdown measures made it lower than it might have been.” This would be a misleading claim, as there are now multiple published analyses showing that lockdown achieved little or nothing –a sample set collated here: https://www.dropbox.com/home/LOCKDOWN NO GOOD - STUDIES
Another key point is that this virus should
never have been compared to the 1918 Spanish Flu. Below data from Sweden shows the difference in scale, in terms of impact per million people:

Note also how the actual Covid19 impact in Sweden is barely discernible from that of influenzas in many months during previous years. Note also that the so-called “second wave” of 1918 Spanish Flu is widely accepted to have been a different virus from the one which caused the first (Spring) wave. An entirely different demographic was impacted during the second wave. Most likely it was resurgence of a tough influenza strain from the 1870’s – hence the older people in the population were spared, while the younger ones with no immunity were hit the hardest.
B2: IMMUNOLOGY REALITIES:
Points from Emeritus Professor of Immunology, Beda Stadler (Switzerland)
The virus is indeed new, as all previous new viruses were “new”. However, it (unsurprisingly) shares many structural properties with prior coronaviruses in this family
It is now clear through many publications over past months that our immune systems recognize these priorly present protein structures when exposed to Sars-CoV-2 leading to a very large extent of immunity in our population from the get-go
This explains the fact that the virus has not come within a mile of the mortality projections of ICL etc. – as in the population it very rapidly “stumbles upon the myriad people who are essentially immune/protected already” – this is “cross-immunity” from prior coronaviruses, and is widespread in the population
He is emphatic that once the virus has passed through its natural cycle, then a population has de facto herd immunity protection – even though only maybe ~10% of people will show positive in an antibody test.
He explains that that is why the mortality and ICU loading has collapsed across most/all of Europe – it is clearly the passing of the susceptible, the development of de facto herd immunity, and also some seasonal mechanisms. But in any case, this is over in Europe until next winter, where more susceptible people will be seasonally affected.
Final key point – contact tracing of symptomatic Covid patients through their direct family members whom they share houses with – shows 70% or more never exhibit infection or symptoms. This illustrates Professor Stadler’s point i.e. the majority of people are ALREADY de facto immune, from cross-immunity to prior coronaviruses etc.
Ref: https://medium.com/@vernunftundrichtigkeit/coronavirus-why-everyone-was-wrong-fce6db5ba809
Discussion with Professor Stadler: https://youtu.be/GBRcK-od50Q
B3: MANDATORY MASK REALITIES
Experts in Ireland and around the World were at best sitting on the fence re the use of masks throughout the pandemic, as the empirical evidence backing up their use if anything pointed to very little benefit in viral transmission mitigation. In any case, given the reality described by the experts above, there is no possible scientific justification for mandating masks at the END of an epidemic. If anything, we run the risk that we will impede safe development of further herd immunity dynamics in our population. This mandate, if anything, could put the most at-risk at even greater risk next winter; an ironic outcome not considered by our “experts”.
The following May 2020 publication alone took the time to compile 14 randomized control trials in mask use and viral transmission. It concluded that masks were near-useless as a mitigation measure. However, there are many more publications over the past 30 years which are aligned in concordance with this conclusion. Note that the WHO themselves have been careful to note that they are NOT instructing governments to implement mandatory masks. Thus, the implementation of mandatory masking has clearly become a politically-driven endeavour:

Ref:
https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
B4: SEASONALITY / REGIONALITY REALITIES
The seasonal nature of this virus needs to be debated and properly explained. It appears to follow a seasonal pattern as based on the work of Dr. Edward Hope-Simpson and fits very neatly with his work. Studying the impact of seasonal viruses over 50 years, Hope-Simpson illustrated that the shape of the curves depends heavily on what region of the World is involved.
Still debated, the drivers of viral triggering include latitude, UV flux, human immune system cycles, humidity etc. In any case, this helps to explain the shape of the mortality/impact curves depending on these variables - showing why the virus has spread in certain US states like New York (North Temperate region) versus Florida (North tropical) and why rising cases now in places like Melbourne and New Zealand are expected. This rise in cases in New Zealand should come as no surprise.
Note just one example below with patterns from Hope-Simpson’s book and also some sample countries. Europe locked down in March same as Peru. Brazil however did not lock down – but the Covid curves simply follow the seasonal pattern regardless. In other words, seasonal/regional vectors dominate – similarly in Northern versus Southern USA regions:
 You can download Hope-Simpson’s book here – he spent >50 years researching viral transmission, after setting up the UK’s first influenza transmission research centre - in 1933: https://www.dropbox.com/s/4yda40j4hf9nbad/11th The Transmission of Influenza BOOK.pdf?dl=0
You can download Hope-Simpson’s book here – he spent >50 years researching viral transmission, after setting up the UK’s first influenza transmission research centre - in 1933: https://www.dropbox.com/s/4yda40j4hf9nbad/11th The Transmission of Influenza BOOK.pdf?dl=0